1.
Target lesions
Follow RECIST1.1 rules / preferences.
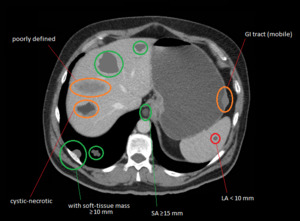
Fig. 2: Drawings over a patient's CT scan.
Example of RECIST 1.1 selection of preferred target lesions (green > orange) and non-measurable lesions (red).
As with RECIST1.1,
all lesions have to be taken into account at baseline.
The excess of measurable lesions and all true non-measurable lesions will be selected as non-target lesions at baseline and followed at subsequent CT scans.
2.
Classic patterns of response
a) CR: disappearance of all target and non-target lesions.
Lymph nodes must decrease to < 10 mm SA (small axis).
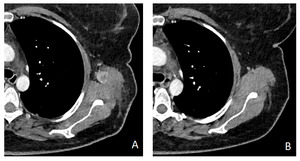
Fig. 3: A. Baseline MDCT of a patient with recidivant unresectable melanoma at scapular region, beginning treatment with Vemurafenib.
B. Within 2 imaging follow-up the lesion is no longer visible, and remains missing through the next year.
b) PR: decrease of ≥ 30% SOL (sum of lesions) relative to baseline,
without unequivocal progression of non-target lesions.
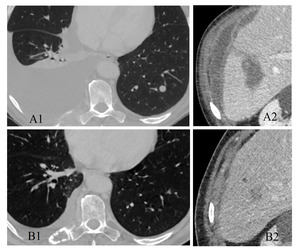
Fig. 4: Patient with stage IV lung cancer, begins treatment with Nivolumab.
A1-2) At baseline MDCT one of the few liver and lung lesions are showed, and there can also be seen non-measurable lesions like carcinomatous right pleural effusion and ascites (confirmed), and a rib metastasis.
B1-2) Follow-up CT after 3 cycles of Nivolumab, an overall improvement of target and non-target lesions is found. Note the sclerotic change of the rib metastasis, sometimes also pointing to response. Total decrease of target-lesions was 52%.
3.
Tumor burden increase
- Increase of ≥ 20% of SOL.
- A follow-up CT in no less than 4-6 weeks is needed,
and a comparison between this new CT scan and the baseline and/or nadir will be made, based on which a final diagnosis ranging from CR to PD can be made.
- Sometimes the clinical worsening that might accompany this increase might be enough to presume progression and avoid the follow-up CT.
- Here are three cases with advanced-stage epidermoid lung carcinoma with one or few target lesions treated with Nivolumab.
In all of them a significant growth was experienced by the tumor (comparing to baseline-nadir); then,
each follow-up CT showed different results:
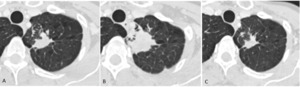
Fig. 5: After a 43% increase, follow-up CT 8 weeks later shows late significant partial response of the only target lesion located in left superior lobe. Patient achieved an even increased degree of partial response in the next CT study.
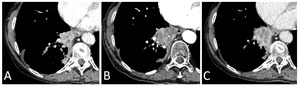
Fig. 6: After a 48% increase, follow-up CT 5 weeks later shows late response of paramediastinal right inferior lobe mass, not meeting neither progression nor significant-response criteria, thus an example of stable disease. Note the relative hypoattenuation (B compared to A) which may also point to some degree of response.
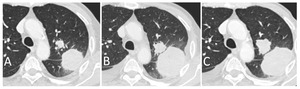
Fig. 7: After a 36% increase, follow-up CT 4 weeks later shows further growth of the main target lesions, therefore confirming progression. Besides, patient suffered worsening symptoms (correlation between clinical and radiological progression).
4.
New lesions
The presence of new lesions does not define progression.
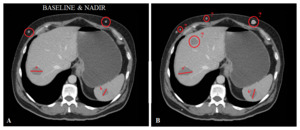
Fig. 8: Drawings over a patient's CT scan.
A previously non-measurable subcutaneus lesion increases its size becoming therefore measurable.
New subcutaneous and liver lesions appear.
- If measurable,
their size will be added to the SOL.
- If not,
they will enter the pool of non-target lesions.
- Previously non-measurable lesions will stay as non-target lesions even if they attain measurable criteria.
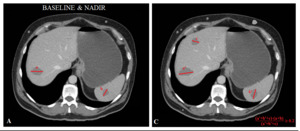
Fig. 9: Same fictional case as Fig.8
The previously non-measurable subcutaneus lesion stays as a non-target lesion even if it has become measurable.
The new measurable liver lesion is added to the tumor burden.
Rest of new lesions (subcutaneous) are not measurable.
If an exploration with new measurable lesions were to experience an increase of ≥ 20% SOL,
even if it is only due to these new measurable lesions,
a follow-up CT in at least 4 weeks may be performed to confirm progression / rule out delayed response.
5.
Non-target lesions
They mostly have a secondary function in tumor evaluation:
- Their continued presence will always prevent the definition of CR.
- As with RECIST1.1,
only a massive and unequivocal increase of non-target lesions (≥70%) might directly indicate progression.
- Any other posibility regarding them is subject to general assessment,
but will not affect PR nor SD categories.
6.
Absence of target lesions
- New measurable lesions will be sought in follow-ups.
- When the first appears,
that CT will serve as baseline as PD might be declared at that time; still sometimes the usual follow-up CT (4-6weeks) might be necessary if clinical status has not also significantly worsened and treatment is in time range for a posible flare effect.
